
The Anesthesia Gas Machine: The One Piece of Equipment You Better Know Cold
Learn how the anesthesia gas machine works. This CRNA-focused guide explains pressure systems, flowmeters, vaporizers, oxygen safety mechanisms, and the critical components every anesthesia provider must understand.
Of all the pieces of technology an anesthesia provider must be intimately familiar with, the anesthesia gas machine tops the list.
It sits quietly in the corner of every OR. It hums. It flashes lights. It looks sophisticated. And yet, at its core, it’s a beautifully organized system of pressure zones, safety mechanisms, vaporizers, and flow controls.
None of the parts are conceptually difficult. But together they can get confusing fast.
Let’s break down the key components every anesthesia provider should truly understand, not just memorize for boards, but actually understand.
First: The Pressure Systems (Where Everything Begins)
The anesthesia gas machine is divided into three pressure systems:
1. High-Pressure System
This is where gas is stored at very high pressures, up to ~1900 psi for oxygen.
It includes:
E-cylinders
Hanger yoke
Cylinder pressure gauges
Check valves
This system deals with tank pressure. It’s powerful. It’s compressed. And it needs regulation before it’s safe to deliver.
(We go deep into this inside our full module, including how failures here present clinically.)
Pressure Regulators: Why 1900 psi Doesn’t Hit Your Patient
Oxygen in an E-cylinder is stored at ~1900 psi.
We obviously cannot deliver that pressure directly to a patient.
That’s the job of the pressure regulator, it reduces cylinder pressure down to about 45–50 psi before entering the intermediate system.
Think of it as the machine’s “shock absorber.”
Without it, nothing downstream survives.
2. Intermediate-Pressure System
This is the “pipeline zone.”
Pipeline gases enter at around 50 psi. This system includes:
Pipeline inlets
Pressure gauges
Oxygen flush valve
Fail-safe valve
Oxygen pressure sensor shutoff valve
This is where oxygen safety mechanisms start to play a major role.
3. Low-Pressure System
This is the most vulnerable part of the machine.
It includes:
Flowmeters (Thorpe tubes)
Vaporizers
Common gas outlet
Gas here is near atmospheric pressure. If there’s going to be a leak, it’s often here.
Understanding where each component lives (high, intermediate, or low pressure) makes troubleshooting infinitely easier.
Oxygen Safety Systems: Hypoxic Guard vs. Fail-Safe Valve
These two are commonly confused, but they do very different things.
The Fail-Safe Valve
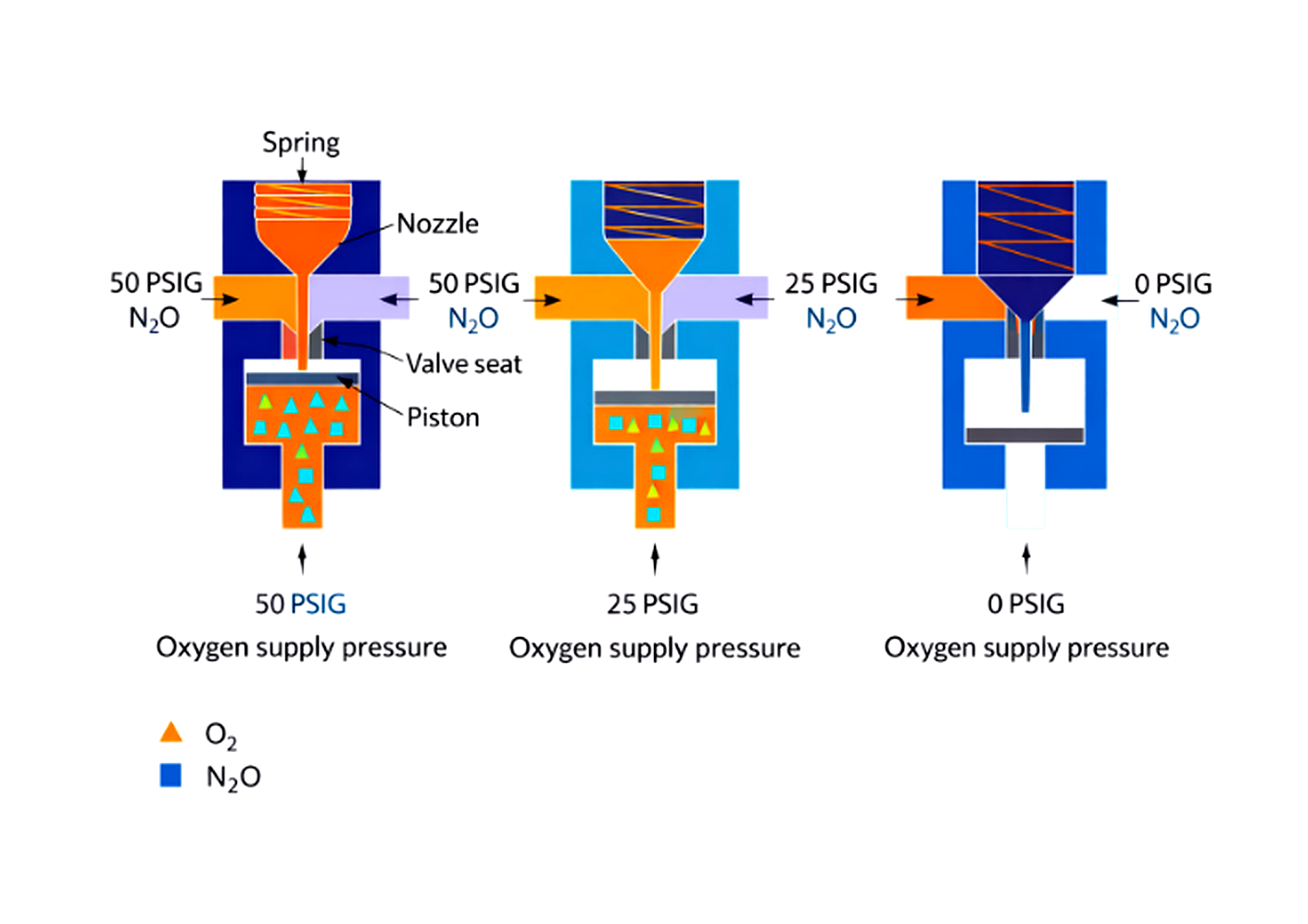
Illustration of anesthesia machine fail-safe valve mechanism demonstrating nitrous oxide shutoff when oxygen supply pressure decreases.
Triggered by low oxygen supply pressure.
If oxygen pressure drops, it reduces or shuts off nitrous oxide flow. It responds to pressure, not oxygen concentration.
Important: It does NOT measure oxygen percentage.
The Hypoxic Guard (Proportioning System)
This links oxygen and nitrous oxide flowmeters to help maintain at least 25% oxygen in the delivered mixture.
It’s mechanical or electronic depending on the machine.
But here’s the key:
It does NOT detect pipeline crossovers. It does NOT analyze oxygen concentration.
That’s why the oxygen analyzer is still your real safety net.
Flowmeters: The Thorpe Tubes

Close-up of an anesthesia machine oxygen flowmeter showing calibrated Thorpe tube used to regulate oxygen delivery.
Flowmeters operate on a variable orifice, constant pressure principle.
The bobbin rises based on flow rate.
Important pearls:
They are gas-specific (density and viscosity matter).
Oxygen flowmeter is placed downstream to reduce hypoxic risk if a leak occurs upstream.
If the bobbin sticks, your flow reading is wrong.
Daily checks matter here.
Variable Bypass Vaporizers
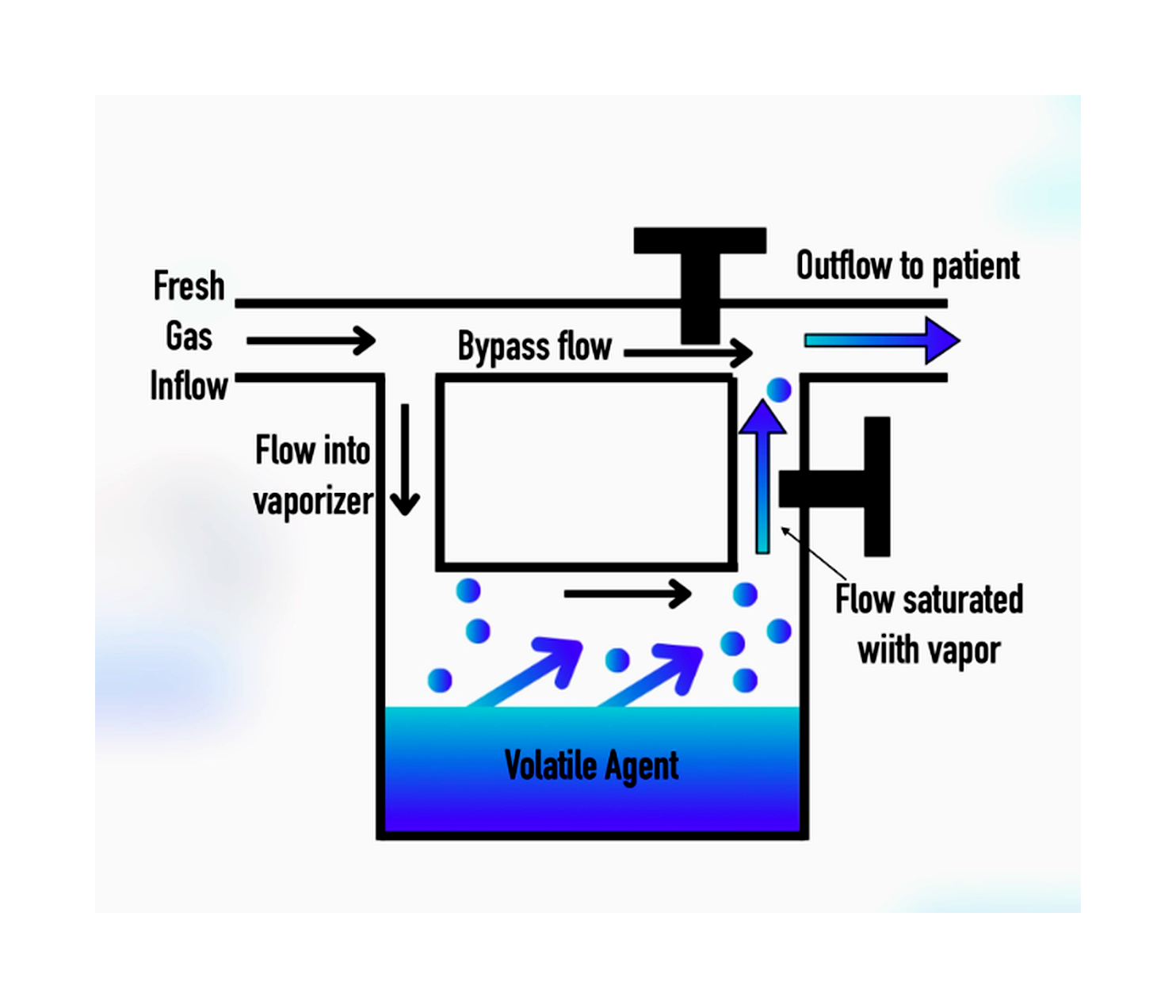
Variable bypass vaporizer diagram showing how fresh gas flow splits between the bypass channel and the vaporizing chamber before exiting to the patient.
For agents like:
Sevoflurane
Isoflurane
The vaporizer splits fresh gas flow:
Some bypasses the chamber.
Some flows through the vaporizing chamber and becomes saturated.
They are:
Agent specific
Temperature compensated
Equipped with interlock systems
Desflurane is different (heated, pressurized system like the Tec 6), but that’s a separate conversation.
The Oxygen Flush Valve: Powerful… and Dangerous
Delivers 35–75 L/min of 100% oxygen directly to the common gas outlet.
It bypasses:
Flowmeters
Vaporizers
Great for:
Rapid circuit filling
Washout
Dangerous if:
Pressed during inspiration
APL valve is closed
Barotrauma is not theoretical.
The Common Gas Outlet (CGO)
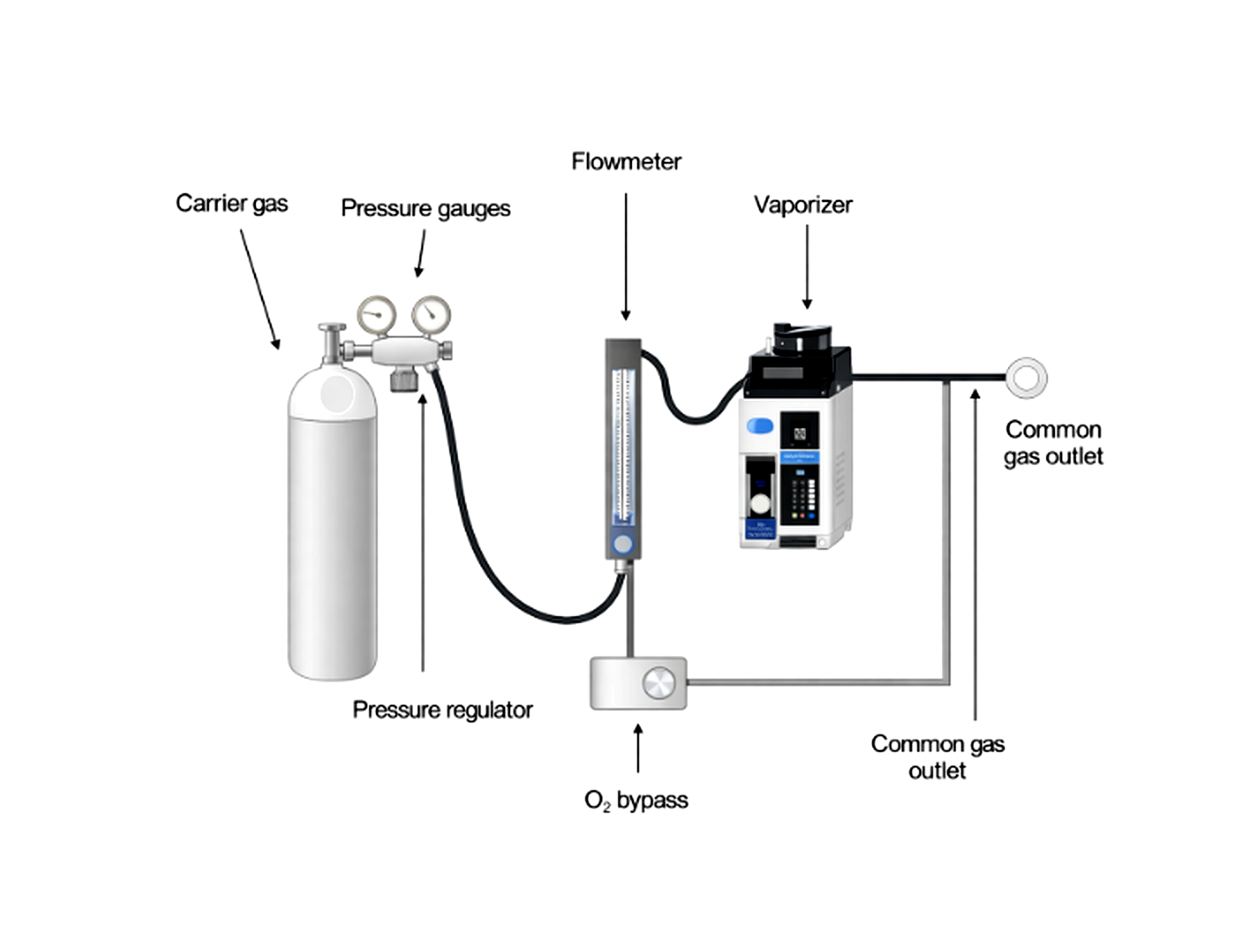
Basic anesthesia machine gas flow pathway showing the carrier gas source, pressure regulator, flowmeter, vaporizer, oxygen bypass, and common gas outlet.
The CGO is the final mixing point before gas enters the breathing circuit.
If this connection is:
Disconnected
Misattached
Accidentally routed to scavenging
You have complete loss of ventilation and anesthetic delivery.
This is why a proper machine checkout is non-negotiable.
Why This Matters clinically
The anesthesia gas machine is not just a test topic.
It is:
Your life-support system
Your oxygen delivery system
Your volatile agent delivery system
Your mechanical ventilator interface
A stuck flowmeter or a pipeline crossover are not just trivia questions, they are real-world failures. If you don’t know how to identify them, it could really cost you and your patient.
Want 1 Class A CE (MAC Check Ed Approved)?
If you want to truly master the anesthesia gas machine, not just skim it, we built a full interactive module inside Ollivate:
“The Anesthesia Gas Machine: A Comprehensive Overview for CRNAs.”
It covers:
Pressure systems
Safety mechanisms (PISS, DISS, hypoxic guard, fail-safe)
Vaporizers (variable bypass vs. Tec 6)
Oxygen flush valve risks
CGO troubleshooting
Breathing circuits
Scavenging systems
Checkout procedures
E-cylinder math
Modern workstation advancements
And it’s worth 1 Class A CE (MAC Check Ed approved).
The first CE is completely FREE.
You can start earning CE while actually learning something that makes you safer in the OR.