
Ketamine vs. Etomidate for Rapid Sequence Intubation: What the Latest Evidence Actually Says
Ask a room full of anesthesia providers which induction agent they prefer for a rapid sequence intubation (RSI), and you will rarely get a quiet, unanimous answer. Ketamine and etomidate both have loyal followings, and for good reason. Each brings real strengths to the table, and each carries a downside that matters in exactly the patients who are sickest.
So which one is actually better? Two recent studies, one published in the New England Journal of Medicine and one in JAMA, set out to answer that question by looking at hemodynamic stability during induction and mortality roughly a month later. The findings are worth understanding, but as you will see, they do not exactly hand us a tidy conclusion.
Let's walk through the pharmacology first, then look at what the evidence shows.
Why Clinicians Reach for Ketamine
Ketamine has a few qualities that make it appealing in a tenuous airway. Among induction agents, it tends to preserve respiratory drive and airway reflexes better than most. That means patients are more likely to keep breathing on their own, which can feel reassuring when you are not certain you will get the tube on the first attempt.
It is worth being honest about a caveat here, though: in a true RSI where a neuromuscular blocking agent is part of the plan, that preserved respiratory drive becomes largely moot. The paralytic is going to take over regardless. So the airway-reflex advantage matters most in scenarios where you are intentionally avoiding or delaying paralysis.
The Catch with Ketamine
Ketamine is often described as cardiostable, and in many patients it is. It typically supports blood pressure through indirect sympathetic stimulation. But that effect depends on the patient having catecholamines left to release.
In catecholamine-depleted patients (think prolonged septic shock, or major trauma where the sympathetic reserves are already exhausted), ketamine’s direct myocardial depressant properties can take over. At higher doses, this can translate into hypotension rather than the blood-pressure support you were counting on. In other words, ketamine is not universally cardiostable. It is cardiostable until the tank is empty.
Why Clinicians Reach for Etomidate
Etomidate's claim to fame is hemodynamic stability. It produces minimal drop in blood pressure and minimal myocardial depression, which is exactly why it feels so safe when you are intubating an already-hypotensive patient. If the blood pressure is hanging by a thread, etomidate is the agent least likely to push it over the edge during induction.
The Catch with Etomidate
The well-known downside is adrenal suppression. Etomidate inhibits 11-beta-hydroxylase in the adrenal cortex, an enzyme essential for cortisol production. The consequence is that even a single induction dose can blunt the cortisol stress response, and in critically ill patients, that suppression can last up to roughly 24 hours.
Whether that transient adrenal suppression meaningfully changes outcomes has been debated for years. The concern is most pointed in patients who depend heavily on an intact stress response, such as those in septic shock. And that concern is precisely what makes the recent mortality data interesting
What the Recent Studies Found
Both studies examined peri-intubation cardiovascular instability and approximately 28-day mortality, although the exact definitions and study designs differed. They arrived at somewhat different signals.
The NEJM Study (Randomized)
Reference: Casey et al., 2026, NEJM
The randomized data showed similar mortality rates between ketamine and etomidate. The notable difference was in the immediate peri-intubation window: there was more cardiovascular collapse with ketamine, with patients more often requiring vasopressor support around the time of intubation. Despite that early instability, the longer-term mortality between the two groups was roughly the same.
The JAMA Study (Observational)

Reference: Maia et al., 2025, JAMA Network Open
The JAMA study sent a different signal. As an observational analysis rather than a randomized controlled trial, it carries more risk of confounding, but it found higher mortality associated with etomidate, even though etomidate produced less immediate hypotension during induction. That finding is at least consistent with the long-standing concern about adrenal suppression in critically ill patients.
So Why Don't the Studies Agree?
Here is the tension in plain terms. The randomized data shows similar survival but more early hemodynamic instability with ketamine. The observational data suggests a possible mortality disadvantage with etomidate, despite its smoother induction.
That is not a contradiction so much as a reminder of how evidence works. Randomized trials are better at isolating cause and effect; observational data can detect real-world signals but cannot prove causation. When the strongest design (the RCT) shows no mortality difference and a weaker design (observational) suggests one, the responsible read is caution rather than certainty.
The honest bottom line: the debate is not settled. Anyone who tells you it is definitively resolved is probably bringing more conviction than the data currently supports.
Ketamine vs. Etomidate at a Glance
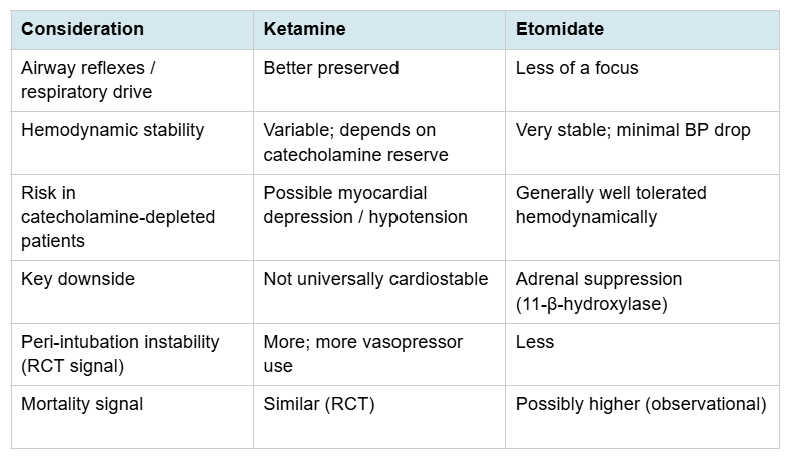
Practical Takeaways for SRNAs and CRNAs
Match the agent to the patient, not the habit. The choice is rarely about which drug is “best” in the abstract. It is about which trade-off your specific patient can least afford.
Respect the catecholamine question with ketamine. In a patient who has been in shock for a long stretch, do not assume ketamine will hold the pressure up for you.
Respect the adrenal question with etomidate. A single dose is usually well tolerated, but in the critically ill, keep the stress-response concern on your radar.
Read evidence by its design. “A study showed” means very different things for a randomized trial versus an observational analysis. That distinction is a clinical reasoning skill, not just an academic one.
Stay comfortable with uncertainty. Sometimes the most accurate answer is “it depends, and the data isn’t settled.” Being able to hold that honestly is part of mature practice.
FAQs
Is ketamine or etomidate better for RSI?
There is no single winner. Randomized data shows similar mortality, with more early hemodynamic instability from ketamine, while some observational data raises concern about higher mortality with etomidate. The right choice depends on the individual patient's physiology.
Why is ketamine not always hemodynamically stable?
Ketamine supports blood pressure largely through sympathetic stimulation. In catecholamine-depleted patients, such as those in prolonged septic shock or major trauma, its direct myocardial depressant effects can dominate, leading to hypotension, especially at higher doses.
What is the main concern with etomidate?
Etomidate inhibits 11-beta-hydroxylase in the adrenal cortex, reducing cortisol production. Even a single dose can blunt the stress response for up to about 24 hours in critically ill patients.
Does preserved respiratory drive from ketamine matter during a true RSI?
Less than you might think. If a neuromuscular blocker is part of the RSI, the paralytic takes over regardless, so ketamine's airway-reflex advantage matters most when paralysis is being avoided or delayed.
Why do the NEJM and JAMA studies seem to disagree?
The NEJM study was randomized and found similar mortality; the JAMA study was observational and suggested higher mortality with etomidate. Randomized designs are stronger for establishing cause and effect, so the discrepancy calls for caution rather than a firm conclusion.
Building the Reasoning Behind the Decision
Notice what this debate is really testing. It is not whether you can recite that etomidate is hemodynamically stable or that ketamine preserves airway reflexes. It is whether you can hold competing pieces of evidence, weigh them against a specific patient, and reason your way to a defensible choice under pressure.
That kind of thinking is exactly what board exams like the SEE and NCE are designed to assess, and exactly what the operating room demands. It is also why Ollivate is built around active recall, spaced repetition, and case-based reasoning rather than passive memorization. The goal is not to help you remember that two studies exist; it is to help you think clearly when a hypotensive, catecholamine-depleted patient needs a tube and a decision in the next thirty seconds.
When your study process trains judgment and not just recall, debates like this stop feeling like trivia and start feeling like clinical reasoning you can actually use. Explore how Ollivate approaches it at ollivate.com.
References and Further Reading
Casey, J. D., Seitz, K. P., Driver, B. E., Gibbs, K. W., Ginde, A. A., Trent, S. A., Russell, D. W., et al., for the RSI Investigators and the Pragmatic Critical Care Research Group. (2026). Ketamine or etomidate for tracheal intubation of critically ill adults. New England Journal of Medicine, 394(16), 1608–1620. https://doi.org/10.1056/NEJMoa2511420
Maia, I. W. A., Decker, S. R. R., Oliveira J. e Silva, L., von Hellmann, R., Alencar, J. C. G., Hajjar, L. A., et al. (2025). Ketamine, etomidate, and mortality in emergency department intubations. JAMA Network Open, 8(12), e2548060. https://doi.org/10.1001/jamanetworkopen.2025.48060
Jabre, P., Combes, X., Lapostolle, F., et al. (2009). Etomidate versus ketamine for rapid sequence intubation in acutely ill patients: A multicentre randomised controlled trial. The Lancet, 374(9686), 293–300. https://doi.org/10.1016/S0140-6736(09)60949-1
Vinclair, M., Broux, C., Faure, P., et al. (2008). Duration of adrenal inhibition following a single dose of etomidate in critically ill patients. Intensive Care Medicine, 34(4), 714–719. https://doi.org/10.1007/s00134-007-0970-y
Albert, S. G., Ariyan, S., & Rather, A. (2011). The effect of etomidate on adrenal function in critical illness: A systematic review. Intensive Care Medicine, 37(6), 901–910. https://doi.org/10.1007/s00134-011-2160-1
Greer, A., Hewitt, M., Khazaneh, P. T., et al. (2025). Ketamine versus etomidate for rapid sequence intubation: A systematic review and meta-analysis of randomized trials. Critical Care Medicine, 53(2), e374–e383. https://doi.org/10.1097/CCM.0000000000006515
This article is for educational purposes for anesthesia professionals and does not constitute clinical guidance for any individual patient. Always follow your institution's protocols and current evidence-based guidelines.